Roux-en-Y Gastric Bypass
Overview
The Roux-en-Y Gastric Bypass, often called the “gastric bypass”, has now been performed for more than 50 years and the laparoscopic approach has been refined since 1993. It is one of the most common operations and is very effective in treating obesity and obesity related diseases. The name is a French term meaning “in the form of a Y”.
The Procedure
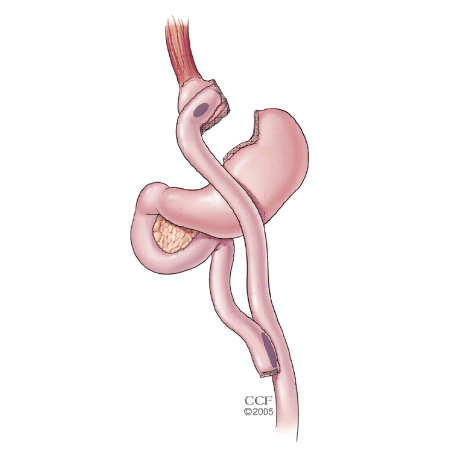
- First, the stomach is divided into a smaller top portion (pouch) which is about the size of an egg. The larger part of the stomach is bypassed and no longer stores or digests food.
- The small intestine is also divided and connected to the new stomach pouch to allow food to pass. The small bowel segment which empties the bypassed or larger stomach is connected into the small bowel approximately 3-4 feet downstream, resulting in a bowel connection resembling the shape of the letter Y.
- Eventually the stomach acids and digestive enzymes from the bypassed stomach and first portion of the small intestine will mix with food that is eaten.
How it Works
The gastric bypass works in several ways. Like many bariatric procedures, the newly created stomach pouch is smaller and able to hold less food, which means fewer calories are ingested. Additionally, the food does not come into contact with the first portion of the small bowel and this results in decreased absorption. Most importantly, the modification of the food course through the gastrointestinal tract has a profound effect to decrease hunger, increase fullness, and allow the body to reach and maintain a healthy weight. The impact on hormones and metabolic health often results in improvement of adult onset diabetes even before any weight loss occurs. The operation also helps patients with reflux (heart burn) and often the symptoms quickly improve. Along with making appropriate food choices, patients must avoid tobacco products and non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen.
Advantages
- Reliable and long-lasting weight loss
- Effective for remission of obesity-associated conditions
- Refined and standardized technique
Disadvantages
- Technically more complex when compared to sleeve gastrectomy or gastric band
- More vitamin and mineral deficiencies than sleeve gastrectomy or gastric banding
- There is a risk for small bowel complications and obstruction
- There is a risk of developing ulcers, especially with NSAID or tobacco use
- May cause “dumping syndrome”, a feeling of sickness after eating or drinking, especially sweets